DEFINITION :
Gynecomastia is defined as an enlargement of the male breast volume.
It can appear as unilateral or bilateral hyperplasia. In some cases it may be related to abnormal hormonesl production, or to certain medications. A mammography or ultrasound can be requested to analyze the density of the gland.
The increase in breast tissue volume in men, especially during adolescence, is often poorly experienced and can cause many psychological disorders.
A surgery may be advised if there is no explanation and the patient feels embarrassed. This surgery is called a « gynecomastia ».
PRINCIPLES :
The goal of corrective surgery is to restore the normal anatomy as well as possible, with the following aims:
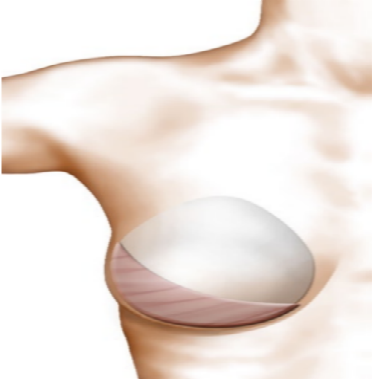
• Reduction of the mammary volume by direct surgical removal (subcutaneous mastectomy) for the glandular forms, or by fat removal for the fat shapes. In the case of mixed shapes, the surgeon will have to combine both techniques.
• Reduction the skin surplus; usually, the decrease in the gland volume will enable the skin to retract. This cutaneous retraction is favored by liposuction. After surgery, some practices such as massages will help the skin retraction.
In some cases, when the skin is too loose, dermal reduction plastie can be performed.
Medical examination in search of a cause to gynecomastia is done systematically. In obese or overweight men, a regimen associated with physical exercises are introduced which can help reduce or even make disappear gynecomastia .
A pre-operative assessment is performed in accordance with the usual requirements.
The anaesthetist will be seen for consultation before surgery.
No medication containing aspirin should be taken within 10 days preceding the intervention.
Stop smoking is essential.
TYPE OF ANAESTHESIA AND HOSPITAL STAY
Type of anaesthesia
This is a classic general anaesthesia during which you sleep completely.
Hospital stay
Hospitalization for 24 to 48 hours is usually required.
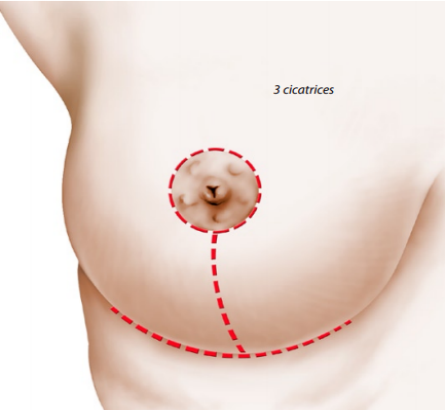
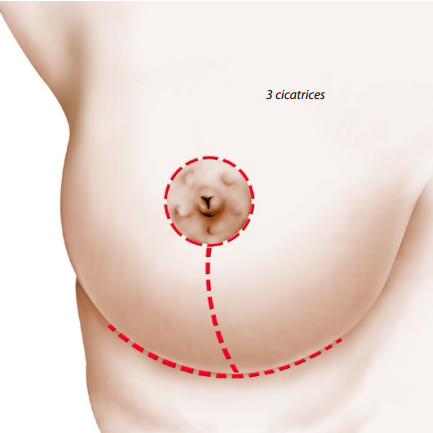
THE OPERATION :
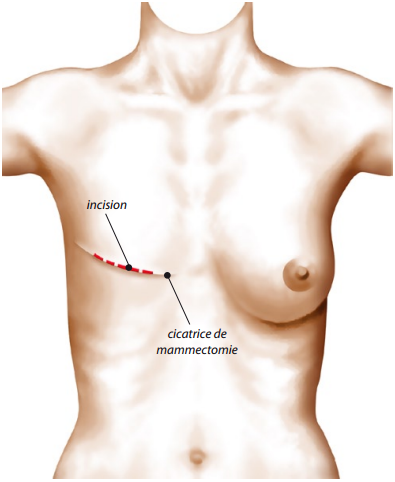
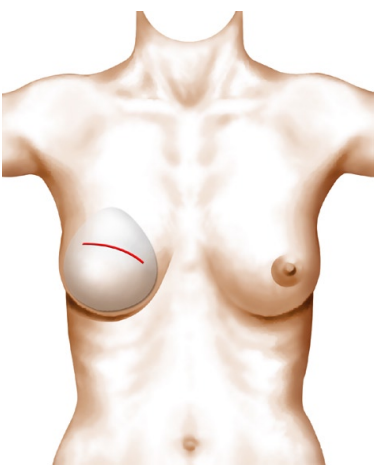
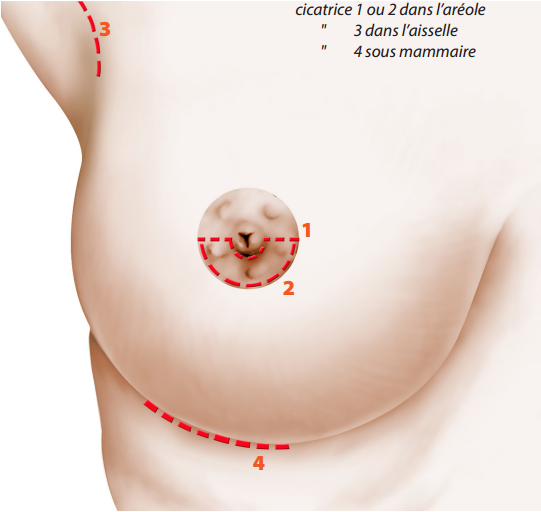
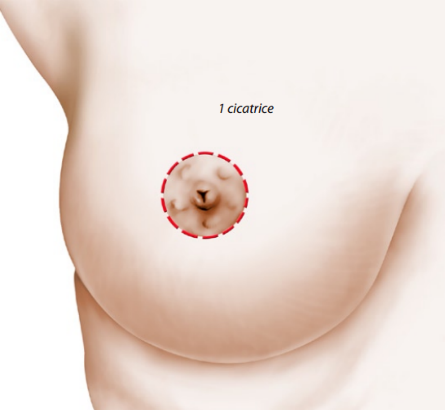
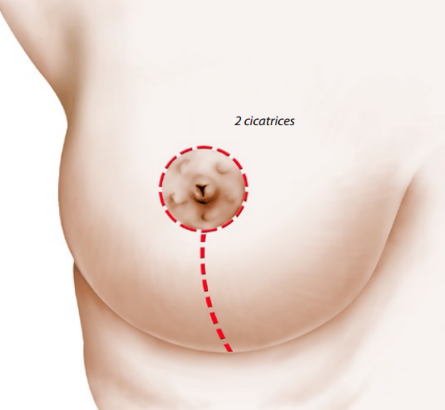
During the surgery, an incision is made in the lower edge of the areola. After this incision, the plastic surgeon can remove the mammary gland and the fat surplus. Often, the plastic surgeon can also perform a liposuction at the periphery of the glandular surplus in order to obtain a harmonious result. If the gynecomastia is important and the skin is too loose, a liposuction can then be performed.
AFTER THE OPERATION : FOLLOW UP
Painkillers will be prescribed according to the pain intensity.
Swelling (edema) and ecchymosis (bruises) in the breasts, and pain on elevation of the arms are frequently observed during the first days.
Often, a pressure bandage is made first, and then, quickly, replaced by a lighter dressing, a kind of support waistcoat to wear day and night for a while. This shall help the skin to retract and make the healing harmonious.
A work leave of 5 to 20 days should be considered. It is advised to wait one to two months to resume a sports activity.
THE RESULT :
However, the final result can not be appreciated before two to three months.
The breast reduction in the tissue volume provides physical comfort, especially when getting dressed. In fact, the result often has psychological benifits.